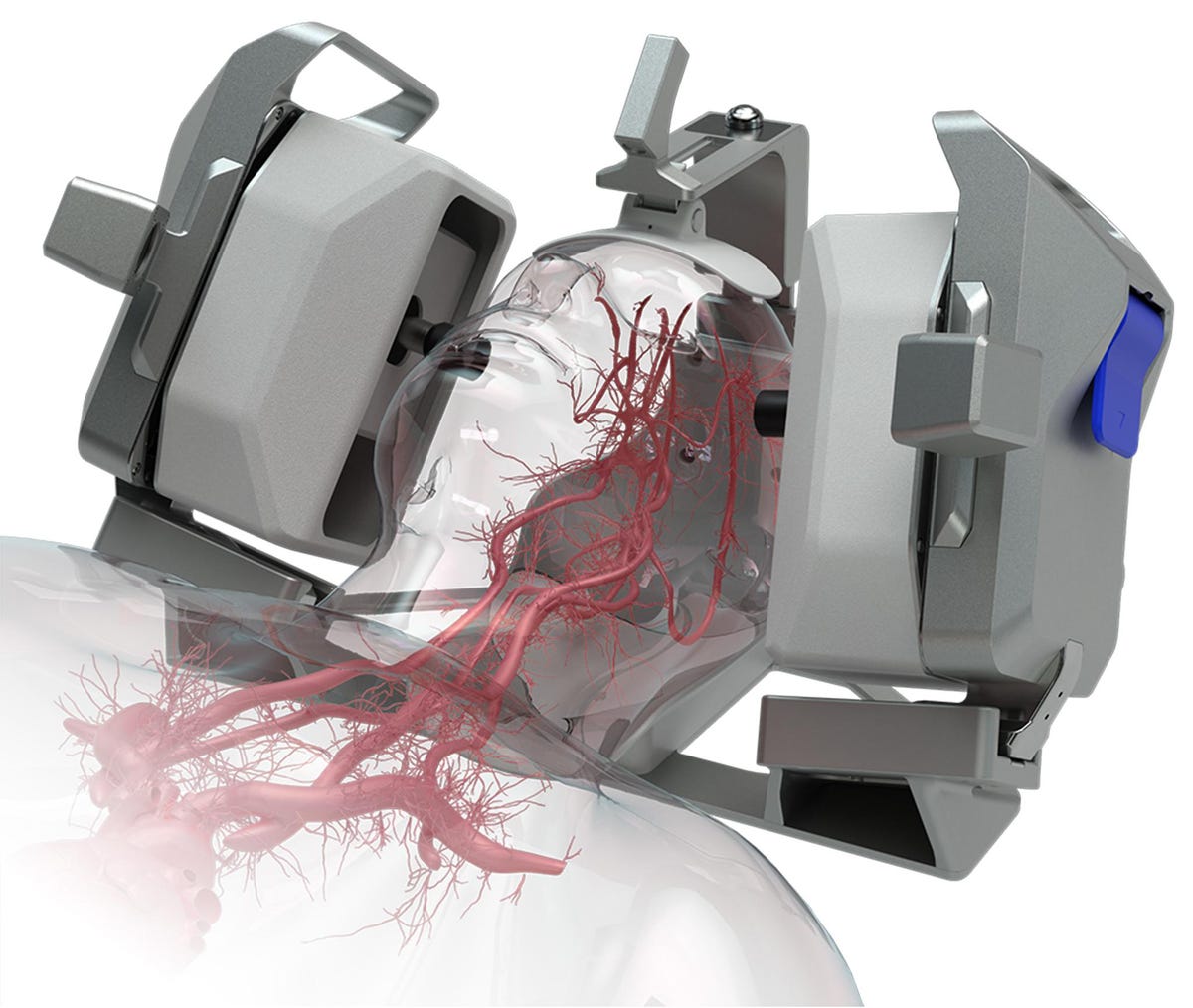
NovaSignal’s AI-driven automated cerebral doppler ultrasound system.
NovaSignal
Los Angeles based NovaSignal Inc. recently launched a second version of their artificial intelligence (AI)-guided robotic platform for assessing cerebral blood flow in order to guide real-time diagnosis. The platform uses ultrasound to autonomously capture blood flow data, which then gets sent to their HIPAA-compliant cloud system so that clinicians can access the exam data from anywhere on their personal devices.
Founded in 2013, the company states they have raised over $25 million in federal research funding and hold 18 patents. They also have over 130 peer-reviewed citations to their work. NovaSignal’s products are FDA-cleared in the United States, CE-marked in Europe, and licensed in Canada.
NovaSignal’s CEO Diane Bryant, and Chief Scientific Officer and co-founder Robert Hamilton, Ph.D. provided their thoughts on where the company started, where it is headed, and what they hope to achieve.
Bryant: At the highest level, our mission is to really change brain health management and to end diseases that present themselves in the brain – like stroke, dementia, Alzheimer’s, and Parkinson’s – but we’re starting with stroke.
Hamilton: The formation of NovaSignal is really the culmination of a number of fortunate accidents and opportunities. It all started with my graduate work at UCLA. And although my technical background was in machine learning and signal processing, all of my engineering work and research was performed in the neuro critical care unit. So I had the opportunity to work with the physicians and neurosurgeons. And while there, my graduate work focused on cerebral blood flow, and do how do we use it for diagnosis, how do we better measure it?
It actually started with a mistake I made in my code very early on where instead of looking at more invasive signals, I actually looked at a noninvasive signal from a new technology at the time called transcranial doppler. I was able to focus on measuring very small changes in cerebral blood flow. And that was really the origin of the company.
The next major nexus for us was when I was asked to go to Africa and help train some U.S. researchers on the use of this technology for cerebral malaria. I realized that due to the extensive training requirements it was impossible to train them in time. So I actually went back to Africa myself a few times to perform the procedure. And those two events, both measuring small variations in blood flow as well as developing a fully automated solution to get that information was really the big motivation.
Bryant: There are multiple usages of the robotic artificial intelligence ultrasound system. If there’s a patient in the ER and there’s suspicion of a stroke, you can put the person into this cradle device. The robot will identify the main arteries in the brain and they’ll be a quick assessment of whether or not a stroke is present, whether or not the blood is flowing to the brain as expected. And that whole process can take less than five minutes. If you look at the statistics, typically from the time you went to the ER to the time you’re treated for a stroke is four and a half hours. And a huge chunk of that is trying to identify if the person is actually having a stroke because there’s no objective way of doing that without an obvious signal.
The second major use case is in the neuro intensive care unit (ICU). If you look at guidelines, once a person has had a stroke and is treated, there’s a 30 percent probability that they will have a second stroke. And so in the neuro ICU, the guidelines state that the patient should be monitored daily for 14 days. The problem is there is no way to continuously monitor that patient. Transcranial doppler itself is a 40 year old technology. It should have should have permeated the healthcare industry. But it hasn’t because of the challenge in using it. It requires a trained neurovascular sonographer and less than 10 percent of the hospitals in the U.S. have such a person. So the daily monitoring of the neuro ICU patient simply isn’t happening. And that’s why patients then are having a recurring stroke.
The third place is in the operating room to monitor cardiac surgery. Cardiac procedures have a very high probability of generating blood clots, which then result in stroke. For some of the more invasive procedures up to 17 percent of patients having open heart surgery will have a lifelong disabling stroke and two percent will actually die of a stroke.
The fourth place is in an outpatient setting. Once you’ve had a stroke, the key is to get to the root cause of the stroke. In an outpatient setting, as well as inpatient, our device is used as an accurate noninvasive, rapid means of identifying a hole in the heart. We’ve been proven to be three times more sensitive with over 90 percent specificity in identifying a hole in the heart to determine whether or not it’s operable.
Hamilton: It’s about access to the information. And that’s what we’re addressing through the robotic system. The nice aspect of building off an existing technology is that the neurologists and neurosurgeons have all been trained on the technology and understand the use cases and its clinical impact. The hurdle has always been access to reliable non-variable information. And so for the applications that we’re selling into today, there’s already an existing knowledge base for those neurologists and neurosurgeons. Democratizing access to that information then allows them to make clinically significant decisions that impact the outcome of their patients.
The first step in the use of artificial intelligence with this technology is really in the delivery of high quality data. The next step is in the interpretation. We are slowly adding assist devices and algorithms to the system that allow physicians to find areas of concern, highlight regions that are important, and provide an analysis for them that is either viewed in the cloud or on a generated report, that allows them to make a more timely, more accurate diagnosis. We’re slowly moving them along the pathway of providing tools driven by machine learning that allow them to do their jobs better and more accurately.
Bryant: It was very intentional to build the technology on transcranial doppler, which already exists in all of the clinical workflows. All medical societies have it in their guidelines. So it’s not that the technology isn’t understood, but without the robotics and AI, it is difficult, if not impossible, for most hospitals to adopt it.
Dr. Chirag Gandhi, Director of Neurosurgery at Westchester Medical Center and Professor and Chair of Neurosurgery at New York Medical College – who is not affiliated with NovaSignal nor has any financial interest in the company – provided an early adopter’s perspective.
Westchester Medical Center is one of the clinical trial centers for the NovaSignal technology. In Dr. Gandhi’s view, some of the key challenges his medical center needed to address in order to do transcranial doppler were the biggest strengths of NovaSignal’s offering. At the top of the list was the ability to reliably and consistently automate much of the process and circumvent a shortage of qualified technologists who can use more traditional doppler ultrasound machines. The same barrier to entry eluded to by Bryant and Hamilton.
Dr. Gandhi and his team also carefully looked at the technology’s safety and how patients responded to it, and the accuracy of the data itself when compared to gold standard clinical protocols for evaluating aneurysms in patients in the intensive care unit.
As with the adoption of any new technology, there were necessary learning curves at times that the clinical team had to address. For example, early on they had issues with the placement and removal of patients’ heads that took some time to properly work through. But after a year of testing they feel confident those early considerations are past them.
More broadly, Dr. Gandhi feels that medicine as a field is moving in a direction where the comfort level and adoption by clinicians of machine learning and artificial intelligence for diagnostic and even treatment considerations is increasing. And for some specific areas, such as neuro-interventional, that adoption is “probably more so than most other fields in medicine [because] it has been blessed with the partnering with engineering, technology and science. If you look at what we can do now compared to even five years ago, it’s a night and day difference. Some of that has been driven by clinical understanding, but a lot of it has been driven by what the engineering teams have been able to build for us to be able to do these things.”
The continued integration of engineering with medicine is not going to slow down anytime soon. In fact, modern medicine is dependent on engineering in a lot of ways. And increasingly, machine learning and AI are contributing to these efforts. Companies like NovaSignal and others are making serious attempts – and being successful – at pushing these boundaries.
Credit: Source link


















{kind=link}